Heroin and its analogues can be deadly. Heroin overdoses have more than tripled over the past couple of decades. The supply has ballooned; the price has plummeted. And, since 2013, dangerous synthetics have hit the streets in truly vast quantities. These are facts, beyond dispute.
Despite this, it has become apparent to me that there is in fact no such thing as an “Opioid Epidemic”. Despite massive reporting and editorializing on the subject, hearings in Congress, and now even a potential military deployment to combat smuggling in the Pacific, there is far more hype than substance, improperly aimed at the medical and pharmaceutical industries. Don’t get me wrong; they’re not blameless, but– No, that’s getting ahead of myself. Read on and I’ll explain this in proper order.
In 2015, the DEA released a report within the annual threat assessment summary. In it they refer to the increasing crisis as an “epidemic” — a political decision designed to help shift the public’s perception of drug abuse from criminal to medical. Which is a good thing overall; we have extensive evidence that imposing even the harshest punishments for drug crimes have little deterrent effect. After all, drug distributors risk death every day at the hands of people who are far less gentle than the American judicial system even at its worst. On the other hand, the medical approach to addiction works even on a national level (as Portugal showed us).
This will seem so very wrong to most Americans. We were raised in the shadow of the drug war, with romanticized criminals like Pacino in “Scarface”, “Breaking Bad”, and the Grand Theft Auto games. We watched Miami Vice, dammit; we know how drug dealers should be handled! Trouble is, that harsh approach, while satisfying, reliably fails. No matter how we try, it just plain doesn’t work.
You don’t have to take my word on it. As I wrote in an earlier article (entitled Stop The War On Drugs — you should read it), “…the Global Commission on Drug Policy released a report which began with the words, “The War On Drugs has failed.” It went on to detail the ineffectiveness of incarceration… and interdiction…”, and it convincingly linked criminalization of narcotics to a highly lucrative political vote grab.
The trend toward medical as opposed to criminal policies on drug use under the Obama administration began shortly after this report was released in 2011, but with very mixed results. It was vigorously opposed by drug enforcement agencies, which if nothing else foresaw this leading to their own eventual obsolescence. And it was resisted in Congress, where “Tough On Crime” has been a vote-winning formula for decades. As a result, very little changed throughout his entire presidency apart from marijuana legalization in some states.
(Which, incidentally, has been highly effective in Colorado. If you’re curious, this is a decent article on the subject — dense, equivocal perhaps, but well worth reading.)
Contemporaneously with this, there’s been a massive increase in heroin production and distribution since the US military began to dominate Afghanistan, and as a matter of policy stabilizing poppies as an export crop (though that policy has since changed under pressure from the U.N.). As a result, the street price across the globe has plummeted and the supply vastly increased; Afghanistan now exports two-thirds of the world’s opium. By curious coincidence, the street market has also been swamped with vast amounts of poorly synthesized non-medical fentanyl, which is so powerful it can kill you just by breathing a little dust.
And you can cook it up at room temperature in your kitchen. (Just, you know, don’t keep it next to the salt shaker.) It’s this widespread availability of non-medical fentanyl analogues that’s the real killer: Without stringent quality controls, you simply can’t rely on street distributors to cut that stuff safely (or as safe as street drugs ever are).
(I just Googled “How do you synthesize fentanyl?” and got an article containing three recipes, a customer feedback study, and street marketing recommendations. On the other hand, I also got a couple of results that were fakes — one with recipes for making yourself very ill, another an obvious tracking-tag plant written by law enforcement. The moral of this story? Don’t try to synthesize fentanyl. Salt shaker, remember?)
Afghanistan is the key here. Just as happened during the conflict in Vietnam, our soldiers overseas are being exposed to common casual drug use as culture in southeast Asia, and they’re picking it up and bringing it home with them. Sometimes literally; though it’s not well-reported, there have been a large number of dishonorable (or the lesser BCD) discharges relating to attempted drug smuggling via military transport.
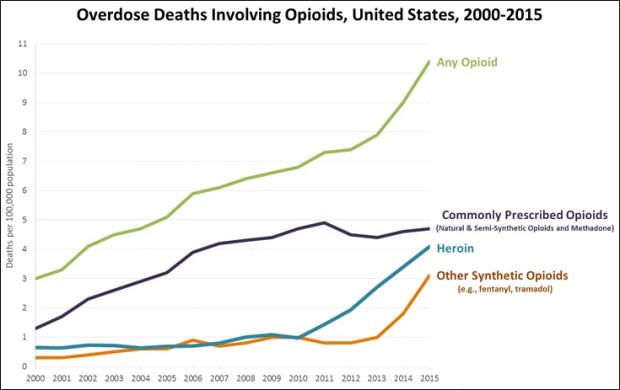
One reason it’s not reported on is that it’s not news; it’s nothing new. With war comes combat; with combat comes wounds, and where there’s wounds there’s painkillers. Most of these are opium-based, and people in pain who’ve also been under the extreme stress of combat are particularly vulnerable to addiction. This factor alone would serve to explain the purple line on the graph at the top of this article, which you’ll note stabilized a decade ago. Given the relatively constant deployment levels, that makes sense.
So what all this tells me is, it’s the decades of war in Afghanistan combined with our policies there that have led us to this pass. Add to this the ready availability of production recipes and the liberties in a free society, and then mix in an ossified economic class system that is perceived to enforce perpetual poverty on our youngest generation, and the end result becomes predictable, even inevitable.
And yet, in the face of this, I’ve said that there is no such thing as an “Opioid Epidemic”. Seems pretty hard to justify, right?
What we have isn’t an epidemic; it’s a concatenation of factors which combine into a spike in the statistics. As an indirect consequence of the U.S. intervention in Afghanistan, the international supply of heroin has approximately tripled since the Taliban banned production in 1999. (International Journal Of Drug Policy) Simultaneously, the recent consolidation of power by the Sinaloa cartel in Mexico combined with an increase in production there has made it even cheaper and well-distributed. The corresponding economic woes in the United States, and a culture of hopelessness that pervades both the inner cities and the new Millennials entering the bottom of the workforce, have worked together to make traffic and use of heroin and its analogues common.
But this is nothing new, merely different. In the eighties, the drug of choice was cocaine; in the nineties, crack; then stimulants; then more recently Ecstasy. Overall drug overdoses have increased, true, but the spike in opiate overdoses is opposed by a sharp decline in every other form of drug use. Some of this stems from painkiller addiction, true, but in large part it’s simply that heroin is more deadly. As the drug use fad evolves, the next product will emerge, and opiate use will decrease proportionately. (Hopefully, the next big thing will be less likely to kill.)
Another factor of great importance is the relative newness of the artificial supply. Street dealers have decades of experience with brick heroin, but non-medical fentanyl is a very new thing indeed. It’s only to be expected that processing will be generally erratic for several years — and, with fentanyl, erratic often means deadly. But drug dealers, particularly the larger organizations, have no wish to kill their customers (quickly), so we can expect improvements to the major pipelines of supply over months rather than years. The amateurs will become a far smaller factor over that same time as customers become informed (and as they pass the salt).
Because of this, it is evident that, far from being a crisis requiring immediate action, what we have is a purely transient spike in activity coinciding with another in fatality. There’ll be loud public outcry for new laws and policies, which, once the natural forces at work in the market take effect, will be trumpeted as having been highly effective. (I’d also suggest that we could enact a government program to simply burn dollar bills wholesale, and that would have a similar impact on opiate overdoses.)
Don’t mistake me: People are dying by the thousands, and it’s tragic; it’s horrific. But it’s not because of a vast increase in drug use; it’s due mainly to a contaminated supply. In a very real sense, it’s because of opiate criminalization: The easiest way to remove contamination from the supply would be to legalize and strictly control production and distribution. Addiction could then be treated on a case-by-case basis as a medical problem. (Again, don’t take my word for that; look at Portugal.) That wouldn’t solve our economic problems, but it wouldn’t hurt; as the price was brought under control, an awful lot of now-unnecessary expenditure nationwide would vanish.
We’re falling victim to a media bias toward sensationalism. The “War On Drugs” is so 1980s, and it failed; the modern medical approach is more effective anyway — which is true, but it has the unfortunate side effect of making the word “epidemic” sexier because somehow scientific. It’s likewise popular to bash Big Pharma, and so we do — even though CDC data clearly shows overdoses are up from heroin and non-medical fentanyl, not medication. “Opium Epidemic” sells; it makes headlines and it attracts votes.
And that means we’re doomed to hear about it over and over even though it isn’t relevant to public policy — at least, we will until the next big thing comes along.
(Graph from CDC, Causes Of Opioid Deaths 2000-15)
